Lipid Profile
Formation of Cholesterol, High-density and Low-density Cholesterol, Principles and procedures of estimation of HDL/LDL, Principle and procedure of estimation of triglycerides, Clinical significance of HDL/LDL/triglycerides estimation, Importance of various ratios of HDL, LDL, and VLDL.
BIOCHEMISTRY
Dr Pramila Singh
11/14/20237 min read
Formation of Cholesterol, High-density, and Low-density Cholesterol, Principles and procedures of estimation of HDL/LDL, Principle and procedure of estimation of triglycerides, Clinical significance of HDL/LDL/triglycerides estimation, Importance of various ratios of HDL, LDL, and VLDL.
Lipid Profile
A lipid profile is a blood test to estimate lipid (fat) levels in blood. It includes cholesterol and triglycerides. Lipid profile helps to assess cardiovascular health and other heart diseases. The following are the parts of the lipid profile
1. Total cholesterol: It includes high-density lipoprotein (HDL or Good Cholesterol) and low-density lipoprotein (LDL or Bad cholesterol).
2. High-density lipoprotein (HDL or Good Cholesterol): It is beneficial for health. It removes cholesterol from the blood circulation to the liver. The liver processes cholesterol to excrete it from the body. It is associated with low heart risk
3. Low-density lipoprotein (LDL or Bad cholesterol): A high level of LDL leads to blocking arteries and the development of heart diseases.
4. Triglyceride: It is a type of fat present in the blood circulation. The body receives it from dietary fat. The human body also synthesizes triglyceride. High triglyceride level is associated with heart disease. Its level increases in obesity, diabetes, and metabolic disorders.
5. Non-HDL Cholesterol: It is total cholesterol minus HDL cholesterol. It estimates the amount of Bad cholesterol in the blood circulation.
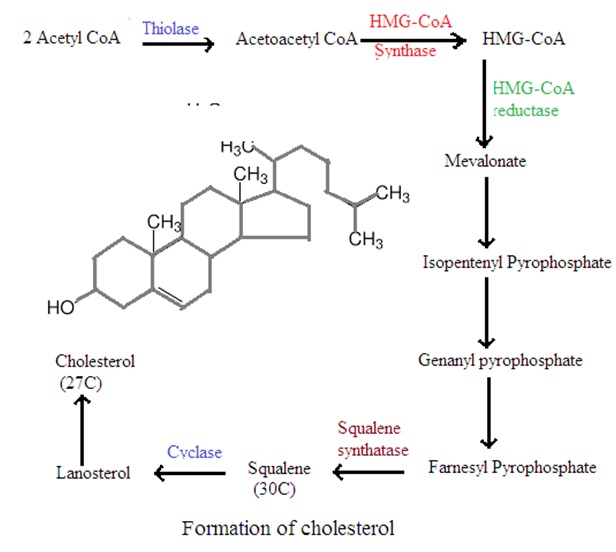
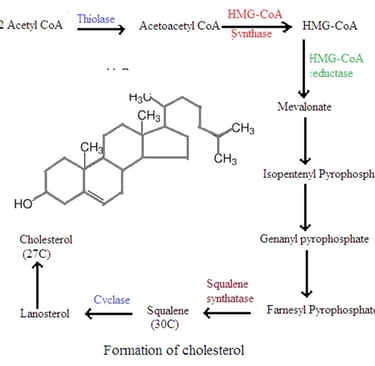
Formation of cholesterol (Cholesterol synthesis or Cholesterol biosynthesis)
90% of Cholesterol biosynthesis inside human occur mainly in the liver and GUT. Cholesterol biosynthesis also takes place in other tissues in very small amounts. Cholesterol inside the human body from dietary sources inhibits hepatic biosynthesis of cholesterol. The human body synthesizes 1.5 to 2 gm/day cholesterol. The human body receives 0.3 gm of cholesterol from the average diet. Cholesterol biosynthesis is a complex procedure. It can be simplified in the following four steps
1. Acetyl Co-A formation: Acetyl Co-A is a two-carbon atom molecule. Acetyl Co-A is derived from carbohydrates, amino acids, and fatty acids.
2. Formation of Mevalonate: Two molecules of Acetyl Co-A condense to form aceto-acetyl Co-A. Aceto acetyl Co-A is a four-molecule compound. Aceto acetyl Co-A again condenses with another acetyl Co-A molecule to form 3-hydroxy-3-methylglutaryl Co-A (HMG Co-A). HMG Co-A is a six-carbon molecule compound. Enzyme HMG Co-A reductase converts HMG Co-a to Mevalonate.
3. HMG Co-A reductase pathways: A series of enzymatic reactions converts mevalonate to isopentanyl pyrophosphate (IPP). IPP is a five-carbon molecule compound.
4. Squalene formation: Several IPP molecules combined to form farnesyl pyrophosphate (FPP). FPP is a 15-carbon molecule compound. Two molecules of FPP combine to form 30 carbon molecules of compound squalene.
5. Cholesterol formation: Series of enzymatic reactions convert squalene to cholesterol.
High-density and low-density cholesterol
High-density lipoprotein cholesterol (HDL Cholesterol): HDL cholesterol is a spherical compound consisting of 50% proteins, 30% phospholipids, and 20% cholesterol. HDL cholesterol transports cholesterol from the periphery blood vessel to the liver. The liver removes cholesterol from the body as bile acid. This process is called reverse cholesterol transport. HDL Cholesterol acts as a scavenger of a lipid such as LDL Cholesterol, VLDL Cholesterol, and other fats. This reduces the risk of artery blockage. Thus HDL cholesterol is called good cholesterol. A high level of HDL cholesterol is associated with a low risk of cardiovascular diseases. A low level of HDL cholesterol is associated with a high risk of cardiovascular diseases.
40 mg/dL HDL cholesterol in men and 50 mg/dL HDL cholesterol in women is considered a healthy level of HDL cholesterol. Normal range is 30 to 60 mg/dL HDL cholesterol in men and 40 to 70 mg/dL HDL cholesterol in women
Low-density lipoprotein cholesterol (LDL Cholesterol): Very low-density lipoprotein (VLDL) cholesterol is synthesized in the liver and released from the liver into blood circulation. Lipoprotein lipase acts on VLDL to form Intermediate-density lipoprotein cholesterol (IDL) and low-density lipoprotein (LDL) cholesterol inside the liver. LDL has 10% cholesterol. LDL enters several cells with blood circulation to participate in cellular function. Too a high level of LDL promotes entry of LDL cholesterol into the artery wall lining. This causes inflammation in the artery wall and formation of plaque. Plaques decrease the diameter of the artery and make the artery wall hard. Plaques tend to block arteries. This develops atherosclerosis and cardiovascular disease. Thus LDL and VLDL are considered as bad cholesterol.
Principles and procedures of estimation of HDL/LDL
Watson method
Principle: LDL VLDL and Chylomicrons precipitated out from the sample by phosphotungstic acid and magnesium chloride. Centrifugation accumulates HDL in supernatant.
Normal values of HDL are 30 to 60 mg/dL HDL cholesterol in men and 40 to 70 mg/dL HDL cholesterol in women.
Reagents
1. Cholesterol reagent 1: 5.6 gm 2,5 dimethyl benzene sulphonic acid in 200 mL of glacial acetic acid and 300 mL of gastric anhydride.
2. Cholesterol reagent 2: Concentrated sulphuric acid.
3. Phosphotungstic acid reagent (PTA):
4. Magnesium chloride reagent:
5. Cholesterol standard: 100mg/dL.
Procedure: Add serum 0.5 mL, PTA reagent 0.05 mL, and MgCl reagent 0.02 mL in a centrifuge tube. Centrifuge it at 3000 RPM for 20 minutes. Separate our supernatant. Prepare test solution, standard solution, and blank solution as per the below details.
1. Test solution: Add cholesterol reagent 2.5 mL, and Supernatant 0.1 mL in cuvette
2. Standard solution: Add cholesterol reagent 2.5 mL, and Cholesterol standard 0.1 mL.
3. Blank solution: Add cholesterol reagent 2.5 mL and distilled water 0.1 mL.
Mix each solution separately and keep in the water bath at room temperature for up to 5 minutes.
Add 0.5 mL cholesterol reagent 2 in each solution. Measure the O.D. of each solution at 575 nm.
Serum HDL Cholesterol mg/dL = O.D. Test solution/ O.D. Standard solution X 114.
Estimation of total cholesterol
Watson method
Principle: Acetic anhydride and cholesterol form a green-colored complex in the presence of glacial acetic acid and concentrated sulphuric acid. The intensity of the green color is proportional to the cholesterol present in the sample. Cholesterol concentration is measured at 575 nm. (green-yellow filter).
The normal range of total cholesterol is 150 to 250 mg/dL.
Reagents
1. Cholesterol reagent 1: 5.6 gm 2,5 dimethyl benzene sulphonic acid in 200 mL of glacial acetic acid and 300 mL of gastric anhydride.
2. Cholesterol reagent 2: Concentrated sulphuric acid.
3. Cholesterol standard: 200 mg/dL.
Procedure: Prepare solution as per the below details
1. Test solution: Add cholesterol reagent 2.5 mL, and Supernatant 0.1 mL in cuvette
2. Standard solution: Add cholesterol reagent 2.5 mL, and Cholesterol standard 0.1 mL.
3. Blank solution: Add cholesterol reagent 2.5 mL and distilled water 0.1 mL.
Mix each solution separately and keep in a water bath at room temperature for up to 5 minutes.
Add 0.5 mL cholesterol reagent 2 in each solution. Measure the O.D. of each solution at 575 nm.
Serum HDL Cholesterol mg/dL = O.D. Test solution/ O.D. Standard solution X 200.
Principle and procedure of estimation of triglycerides
Principle: The following reactions are the basis of serum triglyceride estimation
1. Enzyme lipoprotein lipase converts triglycerides to glycerol and fatty acids
2. Enzyme Glycerol kinase converts glycerol to glycerol-3-phosphate
3. Glycerol phosphate oxidase converts glycerol-3-phosphate in the presence of dihydroxy acetone phosphate and hydrogen peroxide to 4-amino phenazone.
4. Enzyme peroxidize develops a colored complex in the end product of the reaction in the presence of p-chlorophenol.
Reagents
1. Enzyme lipoprotein lipase
2. Enzyme Glycerol kinase
3. Enzyme Glycerol phosphate oxidase
4. Enzyme peroxidise
5. Phosphate buffer pH 7.2
6. p-chlorophenol: 30mg/dL
7. Working reagent: Two parts of reagent 1 to 5 and one part of reagent 6
8. Standard concentration 100 mg/dL
Procedure
Prepare the following solutions in the cuvette
1. Test solution: Working reagent 1 mL and serum sample 0.01 mL
2. Standard solution: Working reagent 1 mL and Standard 0.01 mL
3. Blank solution: Working reagent 1 mL and Distilled water 0.01 mL
Measure the optical density of the test solution and standard solution at 520 nm (green filter) using spectrophotometry.
Calculation
Serum triglycerides mg/dL = O.D. Test/O.D. Standard X 100
Principles and procedures of estimation of LDL
Calculation LDL Cholesterol =
Total Cholesterol – [ Triglyceride/5 + HDL Cholesterol]
Clinical significance of HDL/LDL/triglycerides estimation
HDL, LDL, and triglycerides are important components of the lipid profile. They are used to assess the risk of cardiovascular disease (CVD). It helps to diagnose and manage lipid disorders.
1. HDL: HDL is a good cholesterol. It removes LDL from the arteries. It reduces the formation of plaque in the arteries. HDL clinical significance are
· Cardiovascular protection: HDL transports cholesterol from peripheral tissues and arteries to the liver.
· Low level of HDL is associated with high risk of cardiovascular diseases.
· High level of HDL is cardiac protective
2. LDL: LDL is bad cholesterol. It transports cholesterol from the liver to peripheral tissues and blood in arteries. A high level of LDL develops atherosclerosis and arteries risk of cardiovascular diseases. The following are the clinical significance of LDL estimation
· Atherosclerosis risk assessment: High LDL level increases the risk of atherosclerosis
· Treatment target: Lipid-lowering therapy targets to reduce LDL levels in blood. Low LDL level is associated with a decreased risk of cardiovascular diseases.
3. Triglycerides: Lipids in blood are triglycerides. They are produced by the liver or from the dietary fat. An increase in triglyceride levels is associated with an increase in the risk of cardiovascular diseases. The following are the clinical significance of triglycerides estimation
· Risk assessment: High triglyceride level is associated with obesity, diabetes, insulin resistance, and metabolic syndrome. These all are associated with a high risk of cardiovascular diseases.
· HDL-LDL Relationship: High triglyceride level with low HDL level and high LDL level is more dangerous. It shows a high risk of cardiovascular diseases.
· Medication effectiveness: Medication and change in lifestyles reduces triglyceride level and reduces risk of cardiovascular diseases.
Importance of various ratios of HDL, LDL, and VLDL.
1. VLDL (very low-density lipoprotein): VLDL carries triglycerides from the liver to various cells of the human body. VLDL is the precursor of LDL. Increased VLDL/HDL ratio is a primary risk factor for coronary heart disease. A low level of triglycerides suggests intravascular lipolysis and increased formation of HDL. A high level of triglycerides suggests low intravascular lipolysis and decreased formation of HDL. This is associated with a high risk of atherosclerosis (High atherogenic risk).
2. LDL (Low-density lipoprotein): It is bad cholesterol. A high ratio of LDL/HDL indicates a risk of atherosclerosis (Atherogenic risk) and coronary heart disease.
3. HDL (High-density lipoprotein): It is good cholesterol. It transports excess cholesterol from blood circulation to the liver. The liver excrete excess cholesterol to bile. A high ratio of HDL is beneficial for heart health. It stops atherosclerosis. Thus high HDL/VLDL is good for heart health.
4. A total cholesterol/HDL-cholesterol ratio of less than 5 is good for heart health. A total cholesterol/HDL-cholesterol ratio of more than 5 is bad for heart health. It is associated with a high risk of ischemic heart disease.
Total cholesterol/HDL ratio
· 3.3 to 4.4: Low risk of coronary heart disease
· 4.4 to 7.1: Average risk of coronary heart disease
· 7.1 to 11.0: Moderate risk of coronary heart disease
· More than 11: High risk of coronary heart disease
LDL/HDL ratio
· 0.5 to 3: Low risk of coronary heart disease
· 3.0 to 9: Moderate risk of coronary heart disease
· More than 6: High risk of coronary heart disease
Ratio of HDL, LDL and VLDL provides more clear picture of cardio vascular risk than individual values of HDL, LDL and VLDL level in the human body.